Clinical Images
Darier Disease: Clinical and Dermoscopic Images
1510
Views & Citations510
Likes & Shares
Isolated Polycystic Pancreatic Disease is a rare disease. Asymptomatic cystic lesions is the most common presentation but sometimes it presents with mild vague abdominal pain. Diagnostic evaluation includes abdominal ultrasonography, contrast enhanced computed tomography and/or magnetic resonance imaging. There is scarcity of data on endoscopic ultrasound (EUS) features of isolated polycystic pancreatic disease. Here we are presenting EUS features in a patient of isolated polycystic pancreatic disease.
CLINICAL IMAGE
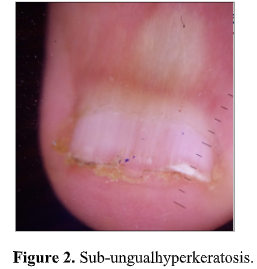
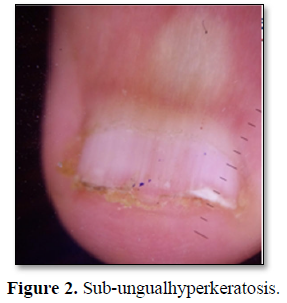
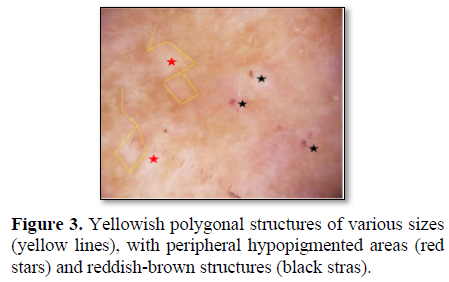
A 41-year-old patient, epileptic since the age of 2, with no family history of hereditary diseases, presented to the dermatology department of our hospital with a 3-year history of persistent pruritic and malodorous papules on the trunk, with excessive sweating in the summer. Physical examination showed brown and hyperkeratotic papules, with a rough and thorny surface and a foul odor, based on homogeneous hyperpigmentation, localized on the seborrheic areas: The trunk and the genital area (Figure 1). He had also sub-ungual hyperkeratosis (Figure 2). There was no mucosal involvement. Dermo copy showed yellowish polygonal structures of various sizes (yellow lines), with peripheral hypopigmented areas (red stars) and reddish-brown structures (black stras) (Figure 3). Systemic examination revealed no abnormalities. Incisional biopsy of the lesions showed characteristic is to pathological findings consistent with the diagnosis of Darier's disease. The patient was treated by urea preparation with a very good course.
Darier disease (DD), or ‘dyskeratosisfollicularis’, is an uncommon autosomal dominant genodermatosis with complete penetrance and variable expressivity [1]. The prevalence of DD is reported to range 1/30 000-100 000, and there is no sex difference. DD maybe accompanied by non-dermal symptoms, including psychiatric symptoms, such as mental retardation, epilepsy or bipolar disease [2]. It mainly manifests as hyperkeratotic, firm papules predominating in seborrheic areas and flexures with associated nail abnormalities. However, it is often under-diagnosed because of the paucity of lesions [3]. The dermoscopic aspects of thisdermatosis are poorlyreported in the literature and can help to guide the diagnosis of Darier’s disease. The most common dermoscopic appearance found a located yellowish/brownish area, surrounded by a more or less thin whitish halo, over lying

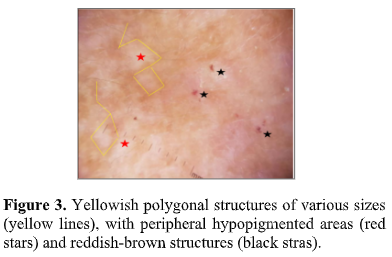
a pinkish homogeneous structure less area [3]. For our patient, dermoscopy showed yellowish polygonal structures with hypopigmented areas and reddish-brown structures.
a pinkish homogeneous structure less area [3]. For our patient, dermoscopy showed yellowish polygonal structures with hypopigmented areas and reddish-brown structures.
- Senhaji G, Jouari OE, Gallouj S, Lamouaffaq A, Mernissi FZ (2018) Lateonse tDarier’sdisease: Clinical and dermoscopic features. J Dermatol Cosmetol 2 : 75-76.
- Takagi A, Kamijo M, Ikeda S (2016) Darier disease. J Dermatol 201643 : 275-279.
- Errichetti E, Stinco G, Lacarrubba F, Micali G (2016) Dermoscopy of Darier's disease. J Eur Acad Dermatol Venereol 30 : 1392-1394.

QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Advance Research on Alzheimers and Parkinsons Disease
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- International Journal of Diabetes (ISSN: 2644-3031)
- BioMed Research Journal (ISSN:2578-8892)
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
")
")



